Destroying the Narrative: 40 Reasons Why a COVID-19 Pandemic Never Existed
“It’s completely understandable that people want to get on with their lives, but we will not be going back to the old normal.”
– WHO Director-General Tedros Adhanom Ghebreyesus
“Many of us are pondering when things will return to normal…The short response is: never. Nothing will ever return to the ‘broken’ sense of normalcy that prevailed prior to the crisis because the coronavirus pandemic marks a fundamental inflection point in our global trajectory.”
– Klaus Schwab, World Economic Forum
The whole world is under the power of an evil spell. The specters of the past like Naziism, Fascism, Communism, and Technocracy are rapidly converging across the globe and hurling us towards a true prison planet where authoritarian rule is commonplace.
None of this would have been possible without State of Emergency declarations being implemented in countries worldwide to stop the so-called coronavirus “pandemic.” Authoritarian governments love emergency powers and executive orders because they provide cover to implement all manner of draconian dictates essentially destroying free speech, freedom of assembly, and freedom of the press all in the name of keeping people safe.
What if the pretext for declaring a pandemic and locking down billions of people was all just a ruse? What if all that’s happened in 202021 had nothing to do with a global health crisis? What if many of the deaths attributed to COVID-19 could have stemmed from other causes? What if the reason for declaring a pandemic was destroy the current world system and institute a “new normal” New World Order?
There is an abundance of evidence suggesting that the coronavirus “pandemic” is nothing but a global social engineering project meant to get people used to obeying mandates and dictates from local, state, federal, and even international powers. The following statement from World Economic Forum leader Klaus Schwab seems to indicate there is indeed another purpose for the crisis:
If it can be proven that there was never a real pandemic, then all instituted measures including lockdowns, masking, social distancing, contact tracing, vaccination, and vaccine passports are totally unnecessary, unethical, unlawful, and must be stopped immediately!
There have been thousands of articles written about the devastating repercussions each one of these “safety” measures has wrought against humanity. This two-part article will tie together many facts that when considered together, will destroy the illusion that humanity ever faced a dire “pandemic.” The list is in no particular order and links to source material are included for reference and further investigation.
Much of this research could not have been achieved without the work of so many independent journalists and alternative media outlets. Now, let’s begin the journey and delve into the 40 Reasons Why a COVID-19 Pandemic Never Existed.
#1 – COVID-19 symptoms are largely indistinguishable from symptoms of other common illnesses.
The CDC’s official list of COVID-19 symptoms do nothing to differentiate COVID-19 from illnesses such as influenza, the common cold, allergies, and pneumonia. Potentially, millions of people diagnosed with COVID-19 likely had one of these other illnesses.
This is readily admitted by mainstream sources and “experts”, who routinely describe “Covid” symptoms as “flu like”.
According to the US Center for Disease Control’s own website comparing “Covid” and the flu:
You cannot tell the difference between flu and COVID-19 just by looking at the symptoms alone because they have some of the same symptoms.
While the UK’s NHS states:
The symptoms [of Covid] are very similar to symptoms of other illnesses, such as colds and flu.
While all mainstream sources couch the admission in soft language – “some of the same symptoms”, “very similar” – the truth is the symptoms are identical. The only points of difference ever observed are equivocations on severity and onset time.
This article from Health Partners highlights that “Covid” can be both more severe OR milder than the flu, noting that “Covid” can sometimes “feel more like a cold”
While according to the Mayo Clinic, in their article on “Covid” vs the flu, the only difference in symptoms is that they “appear at different times”.
A loss of smell and taste is NOT unique to “covid”. As with GGOs, it has been widely reported that a loss of the sense of taste and sense of smell is the telltale sign of “Covid”, but that is a known symptom of many upper respiratory infections.
According to a 2001 article published on the website of the Univerity of Connecticut School of Medicine:
In adults, the two most common causes of smell problems that we see at our Clinic are: (1) Smell loss due to an ongoing process in the nose and/or sinuses such as nasal allergies and (2) smell loss due to injury of the specialized nerve tissue at the top of the nose (or possibly the higher smell pathways in the brain) from a previous viral upper respiratory infection.
Many common medical conditions are known to cause both acute and chronic damage to the sense of smell and taste, according to the UK’s NHS:
Changes in sense of smell are most often caused by a cold or flu, sinusitis (sinus infection) [or] allergies (like hay fever)
#2 – Early test kits developed by the CDC were severely flawed.
A March 2020 article in Business Insider revealed CDC test kits could not distinguish between the coronavirus and water. The CDC had to recall over 32,000 test kits that had been shipped to state public health labs. In April 2020, CDC officials confirmed that COVID-19 test kits sent out to states in February were tainted with the coronavirus. It was determined that sloppy laboratory practices at two of three CDC labs involved in the tests’ creation led to contamination and uninterpretable results. Though it’s said that the tests did not spread coronavirus to people, how do we know this for sure given the multitude of other lies that were told? If you think this was just an issue in the U.S., please see also here, here, and here.
#3 – The RT-PCR test used to diagnose COVID-19 is fraudulent.
It is not possible to clinically diagnose “Covid19”.Clinical diagnosis is the practice of diagnosing a disease based on a unique symptom or collection of symptoms. Wiktionary defines it as:
The estimated identification of the disease underlying a patient’s complaints based merely on signs, symptoms and medical history of the patient rather than on laboratory examination or medical imaging.
Since “Covid19” has no unique symptomatic profile[1], and since ALL major symptoms of “Covid” can potentially apply to literally every common respiratory infection, it is impossible to diagnose “Covid19” based on symptoms.
Lateral flow tests are unreliable. Throughout the “pandemic” the most frequently used “self-test” for “Covid” were Lateral Flow Tests (LFTs). These tests are highly unreliable, and known to return positive test results from household liquids such as fruit juice and soda.
Children in the UK frequently “broke” their LFTs using vinegar or coca-cola in order to create false-positive tests and get a few days off school.
In February 2022, an “expert” told The Guardian that LFTs could create false positives based on the diet of the person being tested, or through “cross-reacting” with a different virus.
In February 2022, it was also reported by a team of “experts” from Imperial College that LFTs can “miss” infectious people. In other words, the official position is that LFTs produce false negative results AND false positive results.
Further, it is acknowledged – and the subject of explainer articles – that LFT and PCR results will often contradict one another. Meaning you can test positive on one, but not the other.
In short, lateral flow tests are of almost no diagnostic value whatsoever.
The late Nobel Prize winning inventor Kary Mullis said that PCRs should never be used for medical diagnosis. The PCR test was never intended to diagnose illness from viruses and current versions cannot distinguish between different coronaviruses or other virus types. The test can only detect the presence of genetic material having a variety of origins. Positivity levels for COVID-19 depend largely on what cycle threshold tests are set for. Anything above 30-35 cycles is likely to produce false positive results. Dr. Anthony Fauci admitted this in an interview from July 2020. According to the New York Times, most U.S. labs set the cycle threshold at 40, meaning test results are highly likely to indicate false positive results.
The late President of Tanzania, John Magufuli, submitted samples of goat, pawpaw and motor oil for PCR testing, all came back positive for the virus.
As early as February of 2020 experts were admitting the test was unreliable. Dr Wang Cheng, president of the Chinese Academy of Medical Sciences told Chinese state television “The accuracy of the tests is only 30-50%”. The Australian government’s own website claimed “There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.” And a Portuguese court ruled that PCR tests were “unreliable” and should not be used for diagnosis.
The unreliability of PCR tests is not unique to “Covid”, either. A 2006 study found PCR tests for one virus responded to other viruses too. In 2007, reliance on PCR tests resulted in an “outbreak” of Whooping Cough that never actually existed.
The CDC is abandoning the current PCR test as of Dec. 31, 2021 citing that a new test will “facilitate detection and differentiation of SARS-CoV-2 and influenza viruses.” This admission implies that the current PCR test cannot make these distinctions! The CDC even admitted that a positive PCR test result does not necessarily indicate that COVID-19 is the definitive cause of disease and may be other bacterial infections or co-infection with other viruses. See also here, here, and here.
#4 – Results from widespread PCR testing led to an increase in false positive “cases” giving the illusion of a pandemic.
death rates were proven to be minimal, the fearmongering campaign focused on the rise of positive “cases”resulting from fraudulent PCR tests. Thousands and potentially millions of people tested positive for COVID-19 though they had no symptoms. Officials and the media were complicit in creating a “casedemic” where healthy people were told they were sick because of a positive test! See also here, here, here, here, here, and here.
The CT values of the PCR tests are too high. PCR tests are run in cycles, the number of cycles you use to get your result is known as your “cycle threshold” or CT value. Kary Mullis said: “If you have to go more than 40 cycles[…]there is something seriously wrong with your PCR.”
The MIQE PCR guidelines agree, stating: “[CT] values higher than 40 are suspect because of the implied low efficiency and generally should not be reported”.
Dr Fauci himself even admitted anything over 35 cycles is almost never culturable.
Dr Juliet Morrison, virologist at the University of California, Riverside, told the New York Times: Any test with a cycle threshold above 35 is too sensitive…I’m shocked that people would think that 40 [cycles] could represent a positive…A more reasonable cutoff would be 30 to 35″.
In the same article Dr Michael Mina, of the Harvard School of Public Health, said the limit should be 30, and the author goes on to point out that reducing the CT from 40 to 30 would have reduced “covid cases” in some states by as much as 90%.
The CDC’s own data suggests no sample over 33 cycles could be cultured, and Germany’s Robert Koch Institute says nothing over 30 cycles is likely to be infectious.
Despite this, it is known almost all the labs in the US are running their tests at least 37 cycles and sometimes as high as 45. The NHS “standard operating procedure” for PCR tests rules set the limit at 40 cycles.
Based on what we know about the CT values, the majority of PCR test results are at best questionable.
The World Health Organization (Twice) Admitted PCR tests produced false positives. In December 2020 WHO put out abriefing memo on the PCR process instructing labs to be wary of high CT values causing false positive results:
when specimens return a high Ct value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain.
Then, in January 2021, the WHO released another memo, this time warning that “asymptomatic” positive PCR tests should be re-tested because they might be false positives:
Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
These announcements coincided with the initial launch of the “covid vaccines”.
The scientific basis for ALL “Covid” tests is questionable. The genome of the Sars-Cov-2 virus was supposedly sequenced by Chinese scientists in December 2019, then published on January 10th 2020. Less than two weeks later, German virologists (Christian Drosten et al.) had allegedly used the genome to create assays for PCR tests.
They wrote a paper, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, which was submitted for publication on January 21st 2020, and then accepted on January 22nd. Meaning the paper was allegedly “peer-reviewed” in less than 24 hours. A process that typically takes weeks.
Since then, a consortium of over forty life scientists has petitioned for the withdrawal of the paper, writing a lengthy report detailing 10 major errors in the paper’s methodology.
They have also requested the release of the journal’s peer-review report, to prove the paper really did pass through the peer-review process. The journal has yet to comply.
The Corman-Drosten assays are the root of every “Covid” PCR test in the world. If the paper is questionable, every PCR test is also questionable.

#5 – The Delta and all other COVID-19 variants are a sham.
The current PCR test can’t differentiate between SARS-CoV-2 and the “Delta” variant (or any variant for that matter). According to the Texas Department of Health and Human Services, “Detecting the Delta variant, or other variants, requires a special type of testing called genomic sequencing. Due to the volume of COVID-19 cases, sequencing is not performed on all viral samples. However, because the Delta variant now accounts for the majority of COVID-19 cases in the United States, there is a strong likelihood that a positive test result indicates infection with the Delta variant.” (Emphasis added).
According to Business Insider, you aren’t legally allowed to know which variant gave you COVID-19 in the U.S., even if it’s Delta. Armed with these facts, how can there be an epidemic of “Delta” variant infections when the PCR test can’t detect it and the required genomic sequencing tests aren’t being performed and haven’t yet been federally approved?
Finally, the supposed Delta variant is no deadlier than the original “SARS-Cov-2” strain. According to a Public Health England report (page 8) from June 18, 2021, the case fatality rate for the Delta variant was 0.1%, about the same rate as the flu.
#6 – Asymptomatic transmission is a myth.
Before the current state of scientific lunacy, you had to actually have symptoms to be diagnosed as being sick from a disease or virus. The COVID-19 “pandemic” turned things around 180 degrees where you could test positive for the virus, but never show any symptoms. A December 2020 study in the Journal of the American Medical Association (JAMA) revealed:
Symptomatic people infect someone else in the house 18% of the time.
Asymptomatic and pre-symptomatic people only infected someone else 0.7% of the time.
The study concluded that “these findings are consistent with other household studies reporting asymptomatic index cases as having limited role in household transmission.” If it’s virtually impossible to contract COVID-19 from someone without symptoms you live with, how is it possible to contract it from interacting with asymptomatic people in public places?
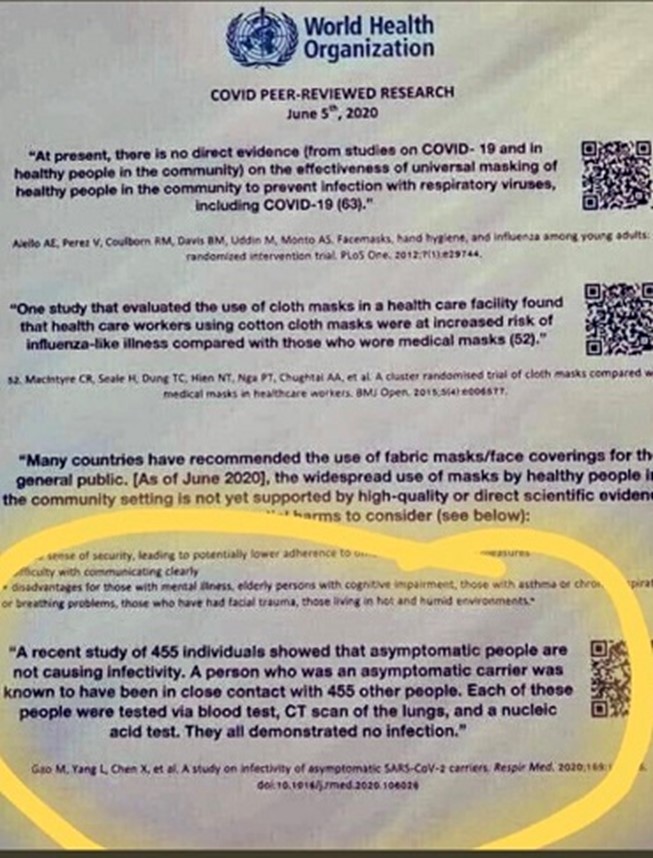
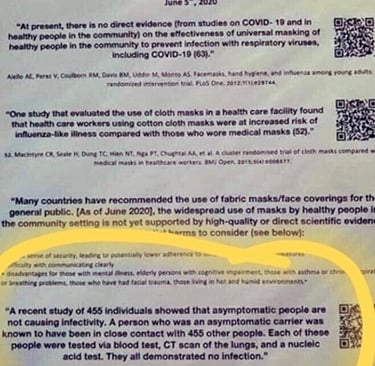
A study by Chinese researchers published by the NIHs National Center for Biotechnology Information (NCBI) revealed that none of the 455 individuals exposed to asymptomatic SARS-CoV-2 carriers for 4-5 days later tested positive for the disease. The study’s conclusion states:
“In summary, all the 455 contacts were excluded from SARS-CoV-2 infection and we conclude that the infectivity of some asymptomatic SARS-CoV-2 carriers might be weak.”
In June 2020, Dr. Maria Van Kerkhove, head of the WHO’s Emerging Diseases and Zoonosis unit publicly stated that asymptomatic carriers very rarely transmit the coronavirus. As this admission began to make major news, Dr. Van Kerkhove and the WHO quickly backtracked, “reassuring” everyone that asymptomatic people can spread the virus. So, which is true? Perhaps the words of Dr. Anthony Fauci (in one of the rare times he’s told the truth) will help clear the confusion, see here. Case closed!
#7 – Over 80% of people who were diagnosed with COVID-19 and placed on ventilators died.
Last year Dr. Cameron Kyle-Sidell sparked controversy with a viral video stating that patients being put on ventilators were dying at an alarming rate. Data from China and NYC indicated that over 80% of people placed on ventilators died. USA Today ran a story stating that most COVID-19 patients put on ventilators die. A Journal of the American Medical Association study from April, 2020 revealed that 88% of New Yorkers placed on a ventilator did not survive. These examples prove that it was medical malpractice that killed thousands of people, not COVID-19.
#8 – Nursing homes and long-term care facilities comprised a large portion of COVID-19 deaths worldwide.
Many of the deaths that created the initial “pandemic” panic were elderly patients in nursing homes and long-term care facilities. In June 2020, USA Today documented 40,600 deaths among nursing home residents and believed this number to be an undercount. The Atlantic corroborated this total and also pointed out that “state and federal officials seem to be doing little to protect the elderly from further devastation.” Former New York Governor Andrew Cuomo should have been held personally responsible for many of these deaths after issuing an executive order allowing COVID-19 positive and infectious patients to be moved to nursing homes for treatment. A May 2020 Guardian article revealed that “90% of the 3,700 people who have died from coronavirus in Sweden were over 70, and half were living in care homes.” In Belgium, more than half of coronavirus deaths were those in care homes. Spain and Italy also had similar numbers.
How many elderly patients truly died from COVID and not some other underlying cause like cancer? Even worse, how many may have been deliberately killed? A damning NHS document revealed that many nursing and care facility patients were potentially given a fatal dose of Midazolam, a drug used for sedation therapy in critically ill patients. See also here.
Were the elderly sacrificed to spark fear and create the illusion that death was imminent if one contracted COVID-19?
#9 – Some COVID-19 patients were denied life-saving medical treatments.
NYC hospitals (at one time the epicenter of the “pandemic” in the U.S.) issued “Do Not Resuscitate (DNR)” orders for dying coronavirus patients. Just as insidious, these DNR orders were also being recommended for those with disabilities. Being denied life-saving treatment goes against the Hippocratic Oath! See also here, here, here, and here.
#10 – Doctors and hospitals were paid more to diagnose patients with COVID-19.
The corruption in our health care system cannot be overstated. According to S. Senator Dr. Scott Jensen, hospitals were given $13,000 for every COVID-19 diagnosis (up from $5,000 for a typical lump sum payment) and $39,000 for every COVID-19 patient using a ventilator by the NIH. Even a USA Today fact check article verified that this was true. This is easily verifiable because the CARES Act authorized increased Medicare payments to hospitals treating COVID-19 victims. Dr. Jensen, who would not go along with the scam was threatened with having his medical license revoked for exposing this truth. In August 2020, former CDC Director Robert Redfield also admitted that hospitals have a monetary incentive to overcount coronavirus deaths.
#11 – The CDC dishonestly mixed in mortality data from pneumonia, influenza or COVID-19 (PIC) to tally death rates.
This overt data manipulation does not present an accurate picture of the death rate for COVID-19 alone. Further evidence can be found in the fact that the flu virtually disappeared. How is this possible? According to a Healthlinereport, “the flu has resulted in 3 million to 49 million illnesses each year in the United States since 2010. Each year, on average, five to 20 percent of the United States population gets the flu.” Creating the PIC category allowed the CDC to hide the flu and relabel it as COVID-19! See also here and here.
#12 – COVID-19 death numbers were inflated.
“Covid deaths” were created by statistical manipulation.Since “Covid” case statistics are inflated [12] it naturally follows that “Covid” death statistics would be likewise unreliable. In fact it was noted from the very beginning of the “pandemic” that “Covid death” counts were being artificially inflated.
According to the UK’s Health Standards Agency, the WHO defined a “Covid death” in the following terms:
A COVID-19 death is defined for surveillance purposes as a death resulting from a clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 disease (eg. trauma).
Throughout the “pandemic” many countries around the globe went even further and defined a “Covid death” as a “death by any cause within 28/30/60 days of a positive test”.
Healthcare officials from Denmark, Italy, Germany, the UK, US, Northern Ireland and others have all admitted to this practice:
A CDC memo dated March 24, 2020 from Steven Schwartz, PhD and Director – Division of Vital Statistics advised coroners and medical examiners to report COVID-19 fatalities for those who did not receive a positive test result as long as it was assumed it caused or contributed to the death.
Montana physician Dr. Annie Bukacek, said “The CDC counts both true COVID-19 cases and speculative guesses of COVID-19 the same. They call it death by COVID-19. They automatically overestimate the real death numbers, by their own admission.”
Dr. Deborah Birx stated that if someone died after testing positive for COVID-19, the death will be counted as COVID-19 even if they died from other causes.


A report showed up to 88% of Italy’s alleged COVID-19 deaths could have been misattributed.
In April 2020, CDC began counting coronavirus cases and deaths not confirmed by lab testing, allowing numbers to be falsely inflated. A U.S. News & World Report article stated that as a result in the change in guidance from the CDC, “There was already a big rise in New York City, where officials this week started counting people who had never tested positive for the coronavirus. That caused the city’s death count to jump by more than 3,700 on Tuesday.”
COVID-19 deaths have been greatly exaggerated from the outset. The CDC has admitted that people who have died from “COVID-19” have had an average of 4 comorbidities, including conditions such as heart failure, diabetes, and cancer. Doesn’t it make sense that one or a combination of these other health conditions led to their death?
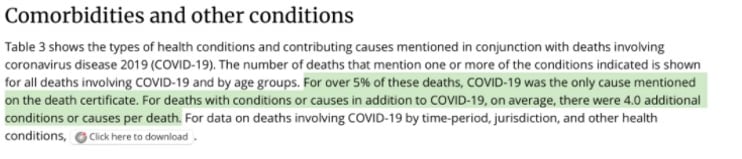
The CDC data also reveals that only over 5% of deaths recorded on official death certificates were attributed solely to COVID-19 as of Sept. 5, 2021. This means that around 95% of recorded deaths were not from COVID-19! See also here, here, here, here, here, here,here, here, here, and here.
Project Veritas exposed the accounts of several directors and workers at New York funeral homes, who admitted that COVID-19 was being written on the death certificate (when it was not the true cause of death) for political and monetary reasons.
The real death rate published by the CDC back in May 2020 is .004% for all ages. This indicates that the survival rate is 99.96% according to their current best estimate at the time. The breakdown is as follows:
0-49: 0.0005
50-64: 0.002
65+: 0.013
Overall: 0.04
The overall survival rate jumped to 99.98% as indicated in the September 10 version of this data. As of this date, the current best estimate for death rates in all age groups was further defined as:
0-19 years: 0.00003
20-49 years: 0.0002
50-69 years: 0.005
70+ years: 0.054
Overall: 0.02
The US CDC even records “probable” Covid deaths in their statistics.
Removing any distinction between dying of “Covid”, and dying of something else after testing positive for Covid will naturally lead to completely meaningless numbers of “Covid deaths”.
British pathologist Dr John Lee was warning of this “substantial over-estimate” as early as April 2020. Other mainstream sources have reported it, too.
Considering the huge percentage of “asymptomatic Covid infections” [11], the well-known prevalence of serious comorbidities [30] and the fact all “Covid tests” are entirely unreliable [II], this renders the “Covid” death numbers a completely meaningless statistic.


#13 – Excess deaths in 2020 were beyond those explainable by COVID-19.
In a March 2021 study, JAMA concluded that “the provisional leading cause-of-death rankings for 2020 indicate that COVID-19 was the third leading cause of death in the U.S. behind heart disease and cancer.” So, with all of the hype and hoopla about a pandemic, more people died from heart disease and cancer as is typical of any other year.
In an article from the BMJ, Dr. John Ioannidis indicated there were several other causes for excess deaths stating, “Under lockdown conditions many patients with acute, treatable conditions (such as coronary syndromes) avoid seeking care. This disruption may be seen in the excess deaths accruing so far in the COVID-19 lockdown. Patients with cancer whose treatment is delayed have worse outcomes. And when patients avoid hospitals many health systems suffer financially, furlough personnel, and cut services. COVID-19 overwhelmed a few dozen hospitals, but COVID-19 Countermeasures have already jeopardized thousands of them.”
The Center for Evidence Based Medicine came to the conclusion that “the total amount of excess mortality [attributed to COVID-19] will also depend on the age structure of a population. Countries with age structures weighted towards an older population will experience higher mortality than a country with an age structure weighted towards a younger population.”
In June 2020, a study revealed that nearly one-third of excess deaths in the early stages of the coronavirus pandemic in the United States were linked to causes other than COVID-19. Study author Dr. Steven Woolf stated, “People who never had the virus may have died from other causes because of the spillover effects of the pandemic, such as delayed medical care, economic hardship or emotional distress.”
Official figures showed there were 2,703 excess deaths across England and Wales as of September 2020, but coronavirus was not even in the top 10 leading causes of fatality. The leading cause of death in September for both countries was dementia and Alzheimer’s disease.
And finally, an article published on Nov. 22 in The Johns Hopkins Newsletter (but deleted a few days later) revealed some startling information about COVID-19 death rates including:
There is no evidence that COVID-19 created any excess deaths. Total death numbers are not above normal death numbers
The total decrease in deaths by other causes almost exactly equals the increase in deaths by COVID-19
Deaths due to heart diseases, respiratory diseases, influenza and pneumonia may instead be recategorized as being due to COVID-19
The CDC classified all deaths that are related to COVID-19 simply as COVID-19 deaths. Even patients dying from other underlying diseases but are infected with COVID-19 count as COVID-19 deaths.
The original article was retracted with an editor’s note on Nov. 27 and made available by PDF.
#14 – In 2009, the corrupt World Health Organization (WHO) changed the definition of a pandemic.
The WHO altered the pandemic definition by deleting “severity of illness” and focusing on the number of cases rather than the number of deaths. Some WHO scientists responsible for creating pandemic policies were being paid by the very pharmaceutical companies creating the vaccines and antivirals that would be used if a pandemic was declared.
The 2009 pandemic definition.
An influenza pandemic occurs when a new influenza virus appears against which the human population has no immunity, resulting in several, simultaneous epidemics worldwide with enormous numbers of deaths and illness.
See also here, here, here, here, here, and here.
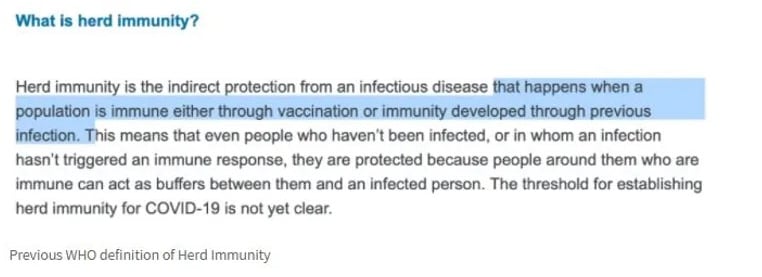
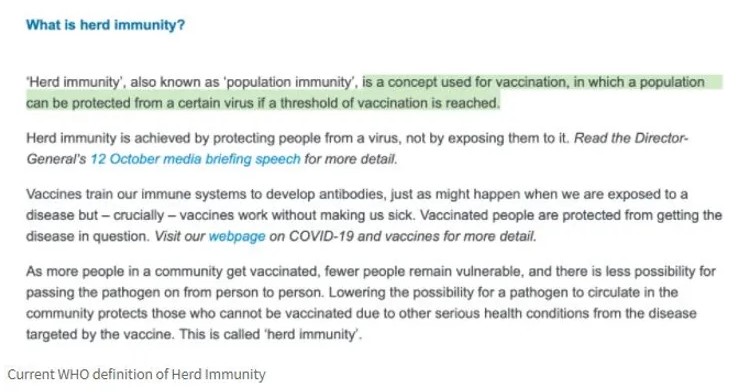
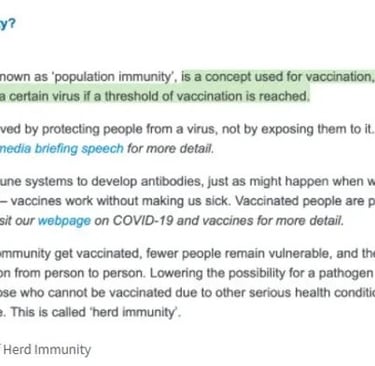
#15 – WHO deleted the references to naturally acquired immunity from its website.
Once known as a basic staple in virology, the definition of herd immunity, also called naturally acquired immunity, was completely redefined by the WHO in a matter of months. No longer did natural immunity mean that a person could be protected from a viral infection because of previous exposure or vaccination; the new definition only emphasized protection from vaccination! The new definition serves to benefit vaccine makers and pigeonholes humanity into seeking protection from vaccines only. See here, here, and here.
In the video below Anthony Fauci, the head of NAID in America states in 2004 that if you get flu and recover that provides better protection than a vaccine.
But during covid they said only the vaccine can protect you and not previous infections.
#16 – WHO Director General Dr. Tedros Adhanom Ghebreyesus, the person who declared a worldwide pandemic on March 11, 2020, is not even a medical doctor!
Ghebreyesus is the first WHO Director not to have this distinction. He is a Marxist Communist who had a key role in leading the murderous communist organization known as the Tigray People’s Liberation Front (TPLF).
In addition, Ghebreyesus was accused of carrying out genocide through forced vaccination, chemical sterilization and abortion, when holding the post of Ethiopian Minister of Health between 2005 and 2012 by the Amhara Professional Union (APU), an Ethiopian civic organization. See also here and here.
To reiterate, the person responsible for declaring a global pandemic and creating mass hysteria and fear to stop an “invisible enemy” is not a medical doctor and is accused of genocide! Where’s the science in that?
#17 – WHO, CDC, and many public health officials confirmed COVID-19 is no more dangerous than the flu.
The survival rate of “Covid” is over 99%. Government medical experts went out of their way to underline, from the beginning of the pandemic, that the vast majority of the population are not in any danger from Covid.
A new global review of Covid data, published in October 2022 by Stanford epidemiologist John Ioannidis (et al) found a median fatality rate of just 0.07% in people younger than 70 years old.
Almost all antibody studies on the infection-fatality ratio (IFR) of Covid have returned results between 0.04% and 0.5%. Meaning, assuming for a moment that “covid” ever existed as a discrete disease at all, its survival rate was at least 99.5%.
During a press conference (below) on April 30, 2020, British Chief Medical Officer Chris Witty, stated, “the great majority of people will not die from this… Of those who get symptoms, the great majority, probably 80%, will have a mild or moderate disease. Might be bad enough for them to have to go to bed for a few days, not bad enough for them to have to go to the doctor.”
One could argue that these statements were made early on before the COVID fatality rate was properly understood. However, the death rate has remained consistent throughout the entire “pandemic” and proves that it has always been more flu like than anything else.
England’s Chief Medical Officer admits “we may have overstated danger of Covid”
England’s Chief Medical Officer testified before the (token and pointless) Covid Inquiry (September 2024), claiming he feared the government “overdid it” when talking up the dangers of Covid.
So if there is little or no real threat why do we all need a vaccine?
During a special session of the WHO’s 34-member executive board on October 5, 2020, WHO officials (inadvertently) revealed that 10% of the world population had been infected with coronavirus. This totaled to about 780 million cases. At the time, the global death toll attributed to COVID-19 was 1,061,539. This would equate to a fatality rate of 0.14%, about the same rate as seasonal flu deaths.
On January 31, 2020, Time published an article entitled “Want to Protect Yourself from Coronavirus? Do the Same Things You Do Every Winter” in which the author wrote, “While 2019-nCoV has never been seen before, it’s part of a family of viruses that are well-known both to doctors and the public; the common cold, for example, can be caused by certain coronaviruses. And while influenza is not a coronavirus, it isn’t so different from 2019-nCoV, either… The things we take for granted actually do work. It doesn’t matter what the virus is. The routine things work.”
On February 1, 2020, USA Today published an article entitled “Coronavirus is scary, but the flu is deadlier, more widespread” in which the author stated, “So far, there have been an estimated 19 million cases of flu, 180,000 hospitalizations and 10,000 deaths in the U.S. this influenza season – including 68 children.”
Dr. Anthony Fauci and former CDC Director Robert Redfield stated, “the overall clinical consequences of COVID-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively” in a published statement by the New England Journal of Medicine on February 28, 2020.
As early as March 19, 2020, Public Health England (PHE) downgraded COVID-19 from the status of a High Consequence Infectious Disease (HCID). This is significant because according to the definition of a HCID, COVID-19 was not acutely infectious, did not typically have a high case fatality rate, or require an enhanced individual, population and system response to ensure it was managed effectively, efficiently and safely.
The vast majority of “covid deaths” have serious comorbidities. In March 2020, the Italian government published statistics showing 99.2% of their “Covid deaths” had at least one serious comorbidity.
These included cancer, heart disease, dementia, Alzheimer’s, kidney failure and diabetes (among others). Over 50% of them had three or more serious pre-existing conditions.
This pattern has held up in all other countries over the course of the “pandemic”. An October 2020 FOIA request to the UK’s ONS revealed less than 10% of the official “Covid death” count at that time had Covid as the sole cause of death.
In summary, the vast majority of “Covid deaths” were very frail people.
This was interpreted by the press as old age or infirmity being “risk factors” for “Covid”. However, it could be more accurately said that the number one risk factor for “dying of covid” was already dying of something else.
Average age of “Covid death” is greater than the average life expectancy. The average age of a “Covid death” in the UK is 82.5 years. In Italy, it’s 86. Germany, 83. Switzerland, 86. Canada, 86. The US, 78, Australia, 82.
In almost all cases the median age of a “Covid death” is higher than the national life expectancy.
Research from March 2021 found that, across the eight studied countries, more than 64% of all “Covid deaths” occurred in people over the national life expectancy.
As such, for most of the world, the “pandemic” had little-to-no impact on life expectancy. Contrast this with the Spanish flu, which saw a 28% drop in life expectancy in the US in just over a year. [source]
#18 – Predictions based on false pandemic models led to lockdowns and harsh measures to “stop the spread” of the “virus.”
On March 16, 2020 the Bill Gates’ funded Imperial College of London model predicted 2 million U.S. deaths and 510,000 in the U.K. In May 2020, this prediction went up in smoke as the mathematical code was deemed sh*tcode. Neil Ferguson, the author of the code/report resigned his position as it was revealed he violated the lockdown by having his married lover visit his home. Governments around the world including the U.S. used this fake computer model to justify strict lockdowns that caused extreme economic hardship, depression, unemployment, and “unintended” negative medical consequences.
#19 – Deborah Birx, former White House Coronavirus Response Coordinator, backed another fraudulent coronavirus model.
The IHME (Institute for Health Metrics and Evaluation) coronavirus model (also funded by Bill Gates) used data from New York and New Jersey (where some of the heaviest concentration of COVID-19 cases were occurring at the time) and applied it to the rest of the U.S., creating a completely false and unrealistic outcome. This prediction was used to further instill fear that death tolls and hospitalizations would drastically rise, further justifying the continuation of lockdowns.
The same IHME predicted that up to 2,800 daily deaths within 11 days and a final death total as high as 75,000 would occur if Sweden didn’t enact strict social distancing measures. For Sweden, the daily death peak was actually 75% lower than the baseline prediction and 96% lower than the worst-case prediction.
#20 – The SARS-CoV-2 virus has never been isolated, only sequenced by a computer.
No government or health agency has proof SARS-CoV-2 exists. FOIA requests from CDC reveal this to be true (FOIA request #21-01075-FOIA). Dr. Andrew Kaufman, Dr. Thomas Cowan, and Sally Fallon Morell have gone on record stating “the SARS-CoV-2 virus has never been isolated or purified. As a result, no confirmation of the virus’ existence can be found.” See also here, here and here, and here.
It’s a global scheme, we’ve been had!
There is no doubt that there was sickness and death occurring throughout the past 18 months that seemed to defy the norm. But can all it be attributed to a virus that in the eyes of many scientists and medical professionals cannot even be proven to exist?
#21 – Hydroxychloroquine was sidelined to make sure vaccines were the only available treatment for COVID-19.
On March 30, 2020 the U.S. Food and Drug Administration (FDA) approved the emergency use of Hydroxychloroquine and Chloroquine to treat COVID-19. On June 15, 2020 the EUA was revoked and the FDA “determined that Chloroquine and Hydroxychloroquine are unlikely to be effective in treating COVID-19 for the authorized uses in the EUA.” This revocation took place despite the fact that the NIH knew Hydroxychloroquine was effective in treating coronaviruses as early as 2005.
Big Pharma stands to gain between $6-$19 billion in revenue from a coronavirus vaccine. Meanwhile Hydroxychloroquine—a proven coronavirus treatment—only costs on average about $20 per bottle.
On May 22, 2020 The Lancet, one of the most reputable medical journals in the world, published a study concluding that Hydroxychloroquine kills more patients and is a dangerous drug.
On June 5, 2020, The Lancet retracted this study after investigations into the company (Surgisphere) providing the data revealed severe inconsistencies and faulty methodology. See more about this unprecedented scandal here and here.
Dr. Anthony Fauci continued to insist that Hydroxychloroquine (an FDA approved drug in use for over 60 years) is not an effective treatment for COVID-19, despite numerous worldwide studies that concluded that it is. Yale epidemiologist Dr. Harvey Risch accused Dr. Fauci of running a ‘misinformation campaign’ against Hydroxychloroquine.
The National Pulse reported that a document no longer available from the FDA regarding “emergency use authorization” of potential COVID-19 treatments appeared to suggest that Hydroxychloroquine satisfied the criteria for the classification, but would have stood in the way of other lucrative drugs and a vaccine.
The American Association of Physicians and Surgeons (AAPS) even sued the FDA for withholding from the public some 60 million doses of Hydroxychloroquine that were donated by drug manufacturers to treat coronavirus patients.
Please see the following list of studies proving that Hydroxychloroquine is an effective treatment for COVID-19 here, here, here, here, here, here, here, and here.
#22 – Props were used to make the “pandemic” look worse than it actually was.
In March 2020, U.S. states and countries around the world began constructing makeshift hospital facilities to accommodate the expected surge of COVID-19 patients. New York anticipated needing an extra 87,000 beds as the Javits Center was converted into a hospital by the Army Corp of Engineers. The U.S.S. Comfort was also deployed to New York City while the U.S.S. Mercy was deployed to Los Angeles. This was all a sham, meant to trick the public into thinking the situation was much more dire than reality. An article in the Navy Times revealed the truth about these makeshift facilities, stating:
By the time of Comfort’s departure, the approximately 1,200-person crew and 1,000-bed hospital had treated just 182 patients, of which approximately 70 percent had COVID-19, according to Capt. Patrick Amersbach, commanding officer of the Comfort’s Medical Treatment Facility.
Underutilization of added medical resources in New York City is not unique to the Comfort. Thousands of hospital beds made available in a converted convention center have gone largely unused after quick assembly by the Army Corps of Engineers.
The Javits Center, which was initially envisioned as a 2,500-bed field hospital for non-COVID-19 patients, converted to coronavirus-only hospital shortly after going operational. Still, the highest number of patients treated at the convention center at one time topped out at close to 500.
Similarly, the U.S.S. Mercy had only treated 77 non-infected patients by the time it departed the port of Los Angeles.
News media were also caught faking stories to stir up fear. CBS This Morning used fake footage to push a story about overcrowded NYC hospitals. The footage was actually from a hospital in Italy. CBS also faked coverage of a testing site in Michigan, with doctors posing as patients lining up in cars to get a COVID-19 test. These are just a couple of examples, but there are dozens more.
Same in the UK Nightingale hospitals where constructed but never used.
UK 500-bed Nightingale Hospital to close without treating a single Covid-19 patient
And all of these hospitals, many of which cost millions of pounds to set up, are either closed or in the process of closing after receiving next to no patients. Meanwhile the government is still threatening the public that the NHS could be overwhelmed at any moment.
London's 4,000-bed Nightingale hospital to be SHUT after treating just 51 Covid-19 patients
#23 – Big Tech, the White House, the media, and governments worldwide joined to censor information.
Facebook, Twitter, Google, LinkedIn, Microsoft, Reddit, and YouTube issued a joint statement about combating fraud and misinformation about the virus, basically admitting collusion to censor views that dissent from the official narrative. In an interview on CNN, YouTube CEO Susan Wojcicki justified censorship of opinions not supported by “authoritative sources,” stating “anything that would go against World Health Organization recommendations would be a violation of our policy. And so, removing information is another really important part of our policy.” Countless individuals, organizations, medical professionals, and political figures were censored, suspended, or completely de-platformed for expressing opinions or citing factual information that poked holes in the story spun by entities like the WHO, CDC, FDA, the White House, and United Nations.
Solving a “pandemic” is not like a mathematical equation where there can only be one right answer. Censorship of differing views and factual information is not a scientific principle, but a totalitarian one that actually violates the scientific method.
#24 – Surprise! COVID-19 doesn’t just infect humans.
Animals including tigers, dogs, cats, gorillas, goats, and even fruit and Coca-Cola all tested positive for COVID-19. Since coronaviruses are very common and were “discovered” in the 1960s, doesn’t this reinforce that these tests are pointless for diagnosing illness, but perfect for creating hysteria and the justification for draconian measures?
#25 – According to real science, face masks do not stop viral transmission.
The wearing of face masks was widely panned in the early months of the “pandemic” by nearly everyone including Dr. Anthony Fauci, former U.S. Surgeon General Dr. Jerome Adams, former CDC Director Robert Redfield, the New England Journal of Medicine, OSHA, and the WHO. A USA Today article from February 2020 documented Fauci’s original stance on masks:
The only people who need masks are those who are already infected to keep from exposing others. The masks sold at drugstores aren’t even good enough to truly protect anyone, Fauci said.
“If you look at the masks that you buy in a drugstore, the leakage around that doesn’t really do much to protect you,” he said. “People start saying, ‘Should I start wearing a mask?’ Now, in the United States, there is absolutely no reason whatsoever to wear a mask.”
In a Dave Rubenstein Show interview in May 2019, Fauci called mask wearing “paranoid” and advised against it as protection against infectious diseases.
An article by Bill Hennessy documented the New England Journal of Medicine’s stance on masks, citing:
For those of you who shout “science” like it’s a Tourette tick, this is from the New England Journal of Medicine on May 21, 2020:
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to COVID-19 as face-to-face contact within 6 feet with a patient with symptomatic COVID-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching COVID-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
So, why are we ordered to wear masks? Symbolism. From the same article in NEJM:
It is also clear that masks serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers’ perceived sense of safety, well-being, and trust in their hospitals.
On April 3, 2020 the initial sentiment around universal masking was reversed when President Trump announced that the CDC recommended that citizens wear cloth face masks in public to stop the spread of the virus. States then began issuing mask mandates even for children, and the controversy about their usage has never gone away.
There have been hundreds of face mask studies. One of the best compilations can be found on Life Site News, where they cite 47 studies that confirm masks are ineffective for COVID-19 and 32 additional studies that confirm they have negative health effects. So, the overwhelming scientific consensus confirms what we were told from the very beginning: masks do not work! Wearing a face mask is nothing more than virtue signaling and blind obedience to today’s scientific cult leaders.
One meta-analysis published by the CDC in May 2020 found “no significant reduction in influenza transmission with the use of face masks”.
A Canadian review from July 2020 found “limited evidence that the use of masks might reduce the risk of viral respiratory infections”.
Another study with over 8000 subjects found masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.”
There are literally too many to quote them all, but you can read them: [1][2][3][4][5][6][7][8][9][10] Or read a summary by SPR here.
In Kansas, counties without mask mandates actually had fewer Covid “cases” than counties with mask mandates. And despite masks being very common in Japan, they had their worst flu outbreak in decades in 2019.
Not only do masks not work, but it was widely known they did not work before 2020.
A 2016 literature review published in the Journal of Oral Health found:
there are no convincing scientific data that support the effectiveness of masks for respiratory protection.
(This study was quietly removed from the journal’s website in June 2020, because it was “no longer relevant in the current climate”.)
Another study, published in 2020 but carried out in 2019, found:
no significant effect of face masks on transmission of laboratory-confirmed influenza.
In his 2020 review, “Masks Don’t Work”, Dr Denis Rancourt cites studies from 2009, 2010, 2012, 2016, 2017 and 2019…none of which found any significant benefit at all from wearing a mask.
And, most tellingly, in their own report on influenza from 2019, the WHO itself noted that: there is no evidence that [masks are] effective in reducing transmission.
A new study (2023) published by Cambridge University Press suggests that wearing a mask may be associated with an increased risk of Covid infection.
From the study,
The crude estimates show a higher incidence of testing positive for COVID-19 in the groups that used face masks more frequently. … The risk was 1.74 (1.38 to 2.18) times higher in those who wore face masks often or sometimes, compared to participants who reported never or almost never wore masks.
In other words, individuals who always or almost always wear face masks have a 75% higher risk of testing positive for COVID-19 than those who never or almost never wear masks.
Health Experts working for governments even said there is NO evidence masks work in April 2020 and you should not wear them. Listen for yourselves. But to keep the Covid fear going among the population during the summer months they decided to advise people to wear masks in July 2020.
#26 – Masks are bad for your health.
Wearing a mask for long periods, wearing the same mask more than once, and other aspects of cloth masks can be bad for your health. A long study on the detrimental effects of mask-wearing was recently published by the International Journal of Environmental Research and Public Health
Dr. James Meehan reported in August 2020 he was seeing increases in bacterial pneumonia, fungal infections, and facial rashes.
Masks are also known to contain plastic microfibers, which damage the lungs when inhaled and may be potentially carcinogenic.
Childen wearing masks encourages mouth-breathing, which results in facial deformities.
People around the world have passed out due to CO2 poisoning while wearing their masks, and some children in China even suffered sudden cardiac arrest.
Moreover, masks may actually increase the likelihood of respiratory disease, a trial of cloth masks from 2015 found that:
Moisture retention, reuse of cloth masks and poor filtration may result in an increased risk of infection.
While a new study published in July 2022 found that masks, especially those worn more than once, were breeding grounds for both bacteria and fungal microbes.
Another peer-reviewed paper on mask effectiveness, from April 2022, found:
While no cause-effect conclusions could be inferred from this observational analysis, the lack of negative correlations between mask usage and COVID-19 cases and deaths suggest that the widespread use of masks […] was not able to reduce COVID-19 transmission. Moreover, the moderate positive correlation between mask usage and deaths in Western Europe also suggests that the universal use of masks may have had harmful unintended consequences.
#27 – Social distancing is a sham.
An article in the UK paper, The Telegraph, stated there is no scientific proof social distancing works and that it is based on very fragile evidence. Even the world-renowned British Medical Journal said social distancing was based on outdated science. Could it really be that social distancing was actually borne from a teenage girl’s science project and adopted as a worldwide policy to keep people apart and afraid of each other?
#28 – Lockdowns do not stop viral transmission, but do destroy people’s lives and the economy.
Stanford Professor Jay Bhattacharya stated, “Itʼs not possible to eradicate (the coronavirus) with a lockdown. We have to come to terms with that… (the lockdown strategy is) doomed to fail and itʼs also going to be counterproductive.”
Prominent medical researcher Knutt M. Wittkowski criticized the lockdown approach saying, “With all respiratory diseases, the only thing that stops the disease is herd immunity. About 80% of the people need to have had contact with the virus, and the majority of them won’t even have recognized that they were infected, or they had very, very mild symptoms, especially if they are children. So, it’s very important to keep the schools open and kids mingling to spread the virus to get herd immunity as fast as possible…”
Lockdowns and staying inside for weeks and months serve to weaken the immune system, say Drs. Dan Erickson and Artin Masseh in Bakersfield, California. The video of the doctors making these statements was censored on YouTube for violating its terms of service.
Studies showed that unemployment caused by lockdowns leads to adverse health effects including stroke, hypertension, heart disease, diabetes, emotional and psychiatric problems, and suicide.
Researchers at Well Being Trust and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care estimated that 75,000 people could die from alcohol, drug abuse and suicide, calling them “deaths of despair.”
The application of lockdowns was arbitrary and inconsistent. Why were liquor and cannabis stores allowed to stay open when churches were forced to close? Why were some businesses (mostly big box stores and major corporations) deemed essential while others were shuttered and forced to apply for government handouts just to survive?
A pre-print meta-analysis from Johns Hopkins University found lockdowns had almost no impact at all on “Covid19” mortality, while another paper on the “Determinants of COVID-19 Fatalities” published in April of 2021 found: little evidence that lockdowns reduced fatalities
Lockdowns kill people. There is strong evidence that lockdowns – through social, economic and other public health damage – are deadlier than the alleged “virus”.
Dr David Nabarro, World Health Organization special envoy for Covid-19 described lockdowns as a “global catastrophe” in October 2020:
We in the World Health Organization do not advocate lockdowns as the primary means of control of the virus[…] it seems we may have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition […] This is a terrible, ghastly global catastrophe.”
A UN report from April 2020 warned of 100,000s of children being killed by the economic impact of lockdowns, while tens of millions more face possible poverty and famine.
Unemployment, poverty, suicide, alcoholism, drug use and other social/mental health crises are spiking all over the world. While missed and delayed surgeries and screenings have already seen increased mortality from heart disease, cancer and other conditions in many countries around the world.
A World Bank report from June 2021 estimated close to 100 million people had been plunged extreme poverty by so-called “anti-Covid measures”.
As of January 2023, healthcare services the world over are still experiencing chaotic backlogs in treatment and diagnosis. The knock-on effects of lockdown will likely hurt public health for years.
The impact of lockdown could account for any observed increases in excess mortality.[
If lockdowns worked, the “pandemic” should have ended as early as summer 2020! Much more could be said on this topic, but I think you get the point.
#29 – Quarantining healthy people is tyrannical and goes against all conventional wisdom.
The Great Barrington Declaration, signed by close to 60,000 scientists and medical professionals and over 800,000 lay people, advised that only the sick should be quarantined. The declaration states, “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.”
Focused Protection has been standard practice for every previous epidemic or pandemic situation. Healthy people should be free to resume normal life and risk exposure. National and regional lockdowns which quarantine the healthy with the sick are nonsensical and have only served to prolong the “pandemic” situation.
#30 – Risk to children is extremely minimal.
A study by Iceland company deCode Genetics revealed that “children under 10 are less likely to get infected than adults and if they get infected, they are less likely to get seriously ill…even if children do get infected, they are less likely to transmit the disease to others than adults. We have not found a single instance of a child infecting parents.”
Data from WorldOMeter showed that children aged 0-17 years have a 0.02-0.06% share of world COVID-19 deaths, which is essentially zero.
A New England Journal of Medicine article advocated for schools to reopen for in person learning, stating “From a clinical standpoint, most children 1 to 18 years old experience mild or no illness from COVID-19 and are much less likely than adults to face severe consequences from the infection.”
Scott Atlas, former member of Trump’s coronavirus task force, stated “We know who is at risk. Only 0.2 percent of U.S. deaths have been people younger than 25, and 80 percent have been in people over 65; the average fatality age is 78.
A JAMA Pediatrics study of North American pediatric hospitals flatly stated that “our data indicate that children are at far greater risk of critical illness from influenza than from COVID-19.”
#31 – Though often vilified, marginalized, and censored, other treatments for COVID-19 exist and are proven to be effective, including:
Vitamin D
Vitamin C
Ivermectin (the human formula, not the horse version)
Budesonide
Nutritional and Oxidative Therapies
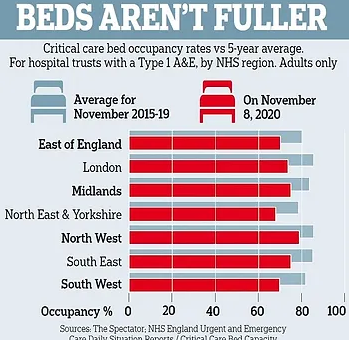
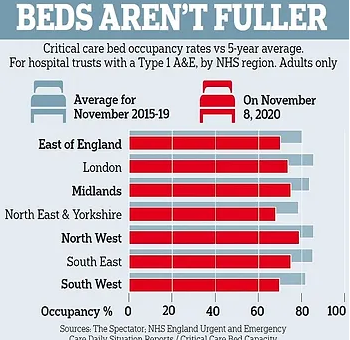
#32 – Hospitals being full to capacity with COVID-19 patients is greatly exaggerated.
Hospitals were never unusually overburdened. The main argument used to defend lockdowns is that “flattening the curve” would prevent a rapid influx of cases and protect healthcare systems from collapse. But most healthcare systems were never close to collapse at all.
In March 2020 it was reported that hospitals in Spain and Italy were overflowing with patients, but this happens every flu season. In 2017 Spanish hospitals were at 200% capacity, and 2015 saw patients sleeping in corridors. A JAMA paper from March 2020 found that Italian hospitals “typically run at 85-90% capacity in the winter months”.
See here, here, here, here, here. As seen from these stories, when hospitals are full, there are many reasons besides COVID-19. The current shortage of nurses due to vaccine mandates is also causing hospital closures, service restrictions and bed shortages.
In the UK, the NHS is regularly stretched to breaking point over the winter.
As part of their Covid policy, the NHS announced in Spring of 2020that they would be “re-organizing hospital capacity in new ways to treat Covid and non-Covid patients separately” and that “as a result hospitals will experience capacity pressures at lower overall occupancy rates than would previously have been the case.”
This means they removed thousands of beds.
Yes, during an alleged deadly pandemic, they actually reduced the maximum occupancy of hospitals.
Despite this, the NHS never felt pressure beyond your typical flu season, and at times actually had 4x more empty beds than normal.
In both the UK and US millions were spent on temporary emergency hospitals that were never used.
An article in Health Policy in November 2021 found that, in all of Western Europe, the “surge capacity” of ICU beds was exceeded for only one day – in Lombardy on April 3rd 2020.
Hospitals were so over ran with covid patients that nurses had time to do TikTok dance routines
#33 – George Floyd protests proved “COVID-19 prevention measures” had nothing to do with public health.
The protests that erupted over the death of George Floyd violated social distancing and, in many instances, mask wearing rules. The protests were encouraged by leftist politicians and mainstream media. Other events where crowds gathered such as the Sturgis Motorcycle Rally in South Dakota or organized lockdown protests were deemed “super spreader” events and widely condemned by these same leftists. This blatant hypocrisy shows that this is a political pandemic more than anything else.
#34 Covid Vaccines
Covid “vaccines” are totally unprecedented. Before 2020 no successful vaccine against a human coronavirus had ever been developed.
Following the advent of “Covid”, we allegedly made over 20 of them in 18 months.
Scientists have been trying to develop a SARS and MERS vaccine for years with little success. Some of the failed SARS vaccines actually caused hypersensitivity to the SARS virus. Meaning that vaccinated mice could potentially get the disease more severely than unvaccinated mice. Another attempt caused liver damage in ferrets.
Whereas the theory behind traditional vaccines is that exposing the body to a weakened strain of a microorganism will trigger an immune response, many of these new Covid “vaccines” are mRNA vaccines.
mRNA (messenger ribonucleic acid) vaccines theoretically work by injecting viral mRNA into the body, where it replicates inside your cells and encourages your body to recognise, and make antigens for, the “spike proteins” of the virus.
mRNA vaccines have been the subject of research since the 1990s, but before 2020 no mRNA vaccine was ever approved for use on humans.
Yet, following the advent of Covid, two different companies made two supposedly “safe and effective” mRNA vaccines within weeks of each other.
“Covid vaccines” do not confer immunity or prevent transmission. It is readily admitted that Covid “vaccines” do not confer immunity from infection and do not prevent you from passing the disease onto others. Indeed, an article in the British Medical Journal highlighted that the vaccine trials were not designed to even try and assess if the “vaccines” limited transmission.
The vaccine manufacturers themselves, upon releasing the untested mRNA gene therapies, were quite clear their product’s “efficacy” was based on “reducing the severity of symptoms”.
In October 2022 Pfizer executive Janine Small, testifying in front of the EU parliament, admitted that Pfizer never even tested if their vaccine prevented transmission of “Covid” prior to its release to the public.
The vaccines were rushed and have unknown long-term effects. Vaccine development is a slow, laborious process. Usually, from development through testing and finally being approved for public use takes many years. The various vaccines for Covid were all developed and approved in less than a year.
Moderna’s own website admits “it normally takes 10-15 years to develop a vaccine”, but boasts of producing their SpikeVax “within 2 months”
Obviously, there can be no long-term safety data on chemicals that are less than a year old.
Pfizer even admits this is true in the leaked supply contract between the pharmaceutical giant, and the government of Albania:
the long-term effects and efficacy of the Vaccine are not currently known and that there may be adverse effects of the Vaccine that are not currently known
Further, none of the vaccines have been subject to proper trials. Many of them skipped early-stage trials entirely, and the late-stage human trials have either not been peer-reviewed, have not released their data, will not finish until 2023 or were abandoned after “severe adverse effects”.
Vaccine manufacturers have been granted legal indemnity should they cause harm. The USA’s Public Readiness and Emergency Preparedness Act (PREP) grants immunity until at least 2024.
The EU’s product licensing law does the same, and there are reports of confidential liability clauses in the contracts the EU signed with vaccine manufacturers.
The UK went even further, granting permanent legal indemnity to the government, and any employees thereof, for any harm done when a patient is being treated for Covid19 or “suspected Covid19”.
Again, the leaked Albanian contract suggests that Pfizer, at least, made this indemnity a standard demand of supplying Covid vaccines:
Purchaser hereby agrees to indemnify, defend and hold harmless Pfizer […] from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses
Covid “vaccines” carry a significant risk of adverse side effects. The experimental Covid vaccines have potentially caused dozens of severe conditions in millions of people. These include myocarditis (especially in young boys), blood clots, allergic reactions, skin conditions, Bell’s Palsy, menstrual irregularities and more. [For a detailed breakdown of these conditions, click here]
The US CDC’s Vaccine Adverse Event Reporting System (VAERS) has received twice as many reports since the covid vaccine rollout than all previous years combined.
Injecting more than half of all humankind with inadequately tested, dangerous pharmaceuticals based on a never-before-tried technology while claiming that that they are “completely safe” constitutes probably the greatest crime against humanity ever committed
The Covid Vaccines are the most dangerous vaccines ever created and have caused more injuries and deaths in 18 months than all other vaccines combined over 30 years for a disease that has a 99.7% recovery rate, which is the same as the flu.
See the following link with a substantial amount of articles and videos about the covid vaccine deaths and injuries:
https://thehardtruth.info/covid-19-vaccines
The covid vaccine doses injected into million were not the same as the doses used in the clinical trials
https://peterhalligan.substack.com/p/dr-john-campbell-learns-that-the
UNFORGIVABLE: CDC confirms 58k Children were Injured, 15k were Hospitalized, 1.2k were left Disabled & 163 tragically Died due to COVID-19 Vaccination in the USA by October 2022
Information request has revealed over 2,100 pages of death reports submitted to the Canadian government following Covid-19 vaccination
Expert Doctor swears 100 million+ Americans may have seriously damaged their Heart due to COVID-19 Vaccination
https://expose-news.com/2023/10/05/100m-americans-serious-heart-disease-covid-vaccination/
Fauci, Walensky and the U.S. government knew that covid jabs were causing myocarditis and blood clots in early 2021, but hid this from the public. The federal government conspired to withhold life-threatening risks on the COVID jab from the public
https://www.thetruthseeker.co.uk/?p=273856
Covid Vaccines are useless. 9 in every 10 COVID Deaths over the last year have been among the Fully/Triple Vaccinated
Legal counsel for covid vaccine injured presented evidence to the UK Covid Inquiry
https://expose-news.com/2023/09/16/legal-counsel-for-covid-vaccine-injured-presented/
Experts estimate over 20 million are already Dead due to COVID-19 vaccination & over 2 billion are Severely Injured
https://expose-news.com/2023/09/15/20m-dead-2b-injured-covid-vaccination/
#35 – There is strong evidence that the coronavirus “pandemic” was pre-planned.
The EU was preparing “vaccine passports” at least a YEAR before the pandemic began. Proposed COVID countermeasures, presented to the public as improvised emergency measures, have existed since before the emergence of the disease.
Two EU documents published in 2018, the “2018 State of Vaccine Confidence” and a technical report titled “Designing and implementing an immunisation information system” discussed the plausibility of an EU-wide vaccination monitoring system.
These documents were combined into the 2019 “Vaccination Roadmap”, which (among other things) established a “feasibility study” on vaccine passports to begin in 2019 and finish in 2021:
This report’s final conclusions were released to the public in September 2019, just a month before Event 201 (below).
In fact, vaccination and immunisation programs have been recognised as “an entry point for digital identity” since at least 2018.
Founded in 2016, ID2020 is a corporate-governmental “alliance”dedicated to “providing digital identity to all”. In March 2018 the ID2020 published an article headlined “Immunization: an entry point for digital identity”, in which the author argues:
Immunization poses a huge opportunity to scale digital identity
ID2020 was founded jointly by Microsoft, the Rockefeller Foundation and GAVI the Vaccine Alliance. Its “partners” include Facebook, and the UN.
A “training exercise” predicted the pandemic just weeks before it started. In October 2019 the World Economic Forum and Johns Hopkins University held Event 201. This was a training exercise based on a zoonotic coronavirus starting a worldwide pandemic. The exercise was sponsored by the Bill and Melinda Gates Foundation and GAVI the vaccine alliance.
The exercise published its findings and recommendations in November 2019 as a “call to action”. One month later, China recorded their first case of “Covid”.
Besides the widely known Event 201 pandemic exercise, governments have been conducting exercises to prepare for a global pandemic for a long time. I have already documented the many exercises, documents, legal proceedings, and conferences that have taken place (please see The Back Story and The Ramp Up from my COVID Chronicles series). Since all this planning has been taking place for at least 20 years, why did everything go so poorly?
#36 – Governments have tried to inflate illnesses into pandemics when not justified before.
See Swine Flu 1976, Zika, SARS 2002-2004, H1N1 2009, and MERS.
#37 –Covid-sceptic world leaders “died suddenly”.
Multiple political leaders who opposed the World Health Organization’s Covid policies died unexpectedly, only to see their anti-WHO covid policies reversed immediately by their successors.
On the 3rd of May 2020, President Pierre Nkurunzia of Burundi dismissed Covid as “a hoax”. Three days later the Council on Foreign Relations warned of “dangerous trends in Burundi’s democracy”.
On May 14th 2020 Nkurunzia formally expelled the WHO representatives from Burundi. Less than a month later, he died “of a sudden illness”. His successor labelled Covid “our biggest enemy”, and invited the WHO back.
There was an almost identical situation in Tanzania, where Covid-sceptic president John Magufuli questioned the accuracy of the PCR tests and banned the use of Covid vaccines in his country.
In March 2021, Magufuli disappeared from public view for weeks. Again, the Council on Foreign Relations published an article calling for his removal, and again it was reported he had died suddenly.
His successor reversed course on Covid immediately, enforcing quarantines, social distancing and mask-wearing, as well as signing Tanzania up to the WHO’s vaccine program and jabbing 10 million of her citizens.
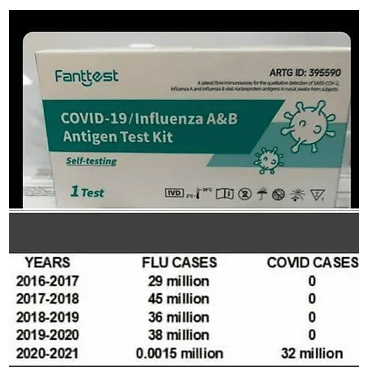
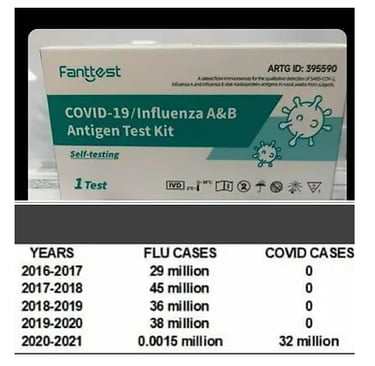
#38 – During the “Covid “pandemic”, the Flu almost completely “disappeared”.
In the United States, since February 2020, influenza cases have allegedly dropped by over 98%.


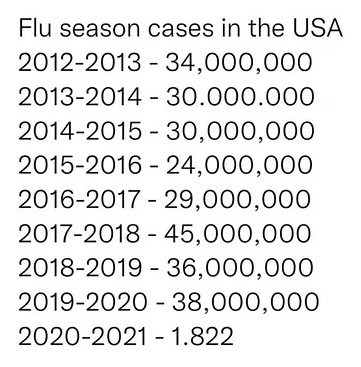
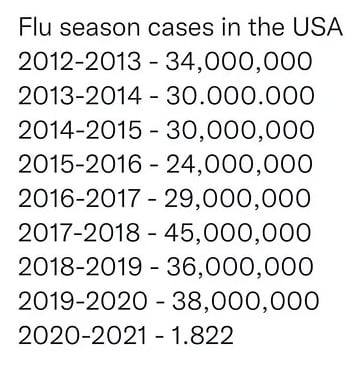
It’s not just the US either, in September 2020 the US CDC reported thatflu activity was markedly decreased in the US, Australia, South Africa and Chile.
In April of 2021, Scientific American published an article headlined:
Flu Has Disappeared for More Than a Year
The explanation given is that anti-Covid measures – eg. masks and lockdowns – stopped flu spreading. But we have established that masks and lockdowns do not halt the spread of respiratory illnesses[14][21].
In short, globally, the flu almost completely disappeared throughout 2020 and 2021, and that cannot be explained by anti-Covid measures.
Meanwhile, a new disease called “Covid”, which has identical symptoms [1] and a similar mortality rate [29] to influenza, was apparently affecting all the people normally affected by the flu.
#39 – The “pandemic” ushered in the rise of authoritarian leadership just as predicted in the 2010 Rockefeller Report (see page 18).
Under the guise of public health and safety, governments committed all kinds of atrocities in the name of keeping people safe. People were arrested for not wearing masks, protesting lockdowns, and not observing social distancing; forced to wear ankle bracelets like criminals for refusing to quarantine; forced to dig graves and get into coffins; kicked off airplanes; forcefully removed from public transportation, spied on by drones and robots; forced to wear masks at home for teleconferences; stopped at quarantine checkpoints; required to use contact tracing apps; constantly surveilled; and left unemployed by the millions from lockdowns.
The Covid pandemic advanced a pre-existing political agenda. From its earliest days, Covid was used as an excuse to push through reforms of food, identity and monetary systems, as well as advance “green” agendas that centralise both global and national power.
As early as March 2020, former UK Prime Minister Gordon Brown was calling for a “global government” to tackle the pandemic.
The pandemic also saw an increase in censorship and surveillance powers, both in China and the West.
In September 2018, the important role of “digital identity” in the future “social contract” was a major talking point at Davos. By December 2020, The Economist reported that “Covid-19 spurs national plans to give citizens digital identities”.
In January 2019, it was reported the Bank of International Settlements and 70 central banks around the world were involved in research on central bank digital currencies (CBDCs). In July 2021 FinTech times reported that the pandemic had “accelerated the development of Central Bank Digital Currencies by up to five years”,
Throughout 2019, articles and papers called for a “radical transformation” of the global food system. By 2021 Deloitte was reporting that “Covid” had “accelerated food transformation”.
The Grantham Institute of Imperial College, London published an article claiming Covid had allowed expert opinion “a foot in the door” so they could “strongly advocate for a ‘net-zero emissions’ recovery and a resilient future.”
Finally, the pandemic opened the door for sweeping globalist changes to public health policies in the form of the proposed “Pandemic Treaty”.
Corporations saw MASSIVE profits due to Covid. Companies in multiple sectors saw huge profits due to the “pandemic”, most of which arose from increases in government spending putting public money in private hands.
The global market for facemasks, for example, expanded by over 15000%, from $1.4 billion in 2019 to $225 billion in 2020. And that’s just facemasks, not other forms of personal protective equipment (PPE) which all saw massive increases in both personal and government spending.
In the UK alone, the cost of simply storing this PPE surged to over 1 billion pounds, with another £4 billion worth of unused PPE simply thrown away, and other write-offs totalling nearly £10 billion.
Rubber gloves and hand sanitzers also saw huge upticks in their market thanks to government spending. A lot of this money was completely wasted as products expired.
Amazon saw its profits double thanks to covid, and streaming platforms added millions of new users thanks to lockdowns
However, the biggest profits were seen in the vaccine sector. Since the vaccine rollout, pharmaceutical companies have made roughly $1000 a second.
In late 2019, Pfizer’s revenues were the lowest they had been since 2010, two years later they had increased by 150%, and were the highest they had ever been.
Within months of the vaccine rollout, 9 vaccine manufacturers had becomes billionaires. By May of 2022, that number had risen to 40.
The elite have made fortunes during the pandemic. It is not just pharmaceutical companies that have profited from Covid, since the beginning of lockdown the wealthiest people have become significantly wealthier.
In October 2020, Business Insider reported that “billionaires saw their net worth increase by half a trillion dollars” in just the first six months of the pandemic.
By April 2021 Forbes was reporting that 40 new billionaires have been created “fighting the coronavirus”.
That process has only accelerated.
As of May 2022, the number of new billionaires created by the pandemic stood at 543. Or roughly one every 30 hours for the previous two years. That includes 40 new billionaires in the pharmaceutical sector alone.
Meanwhile, the share of the world’s wealth held by billionaires has increased from 10% in 2019 to 14% in 2022, a greater increase than the previous 16 years combined.
Altogether, the richest people in the world increased their collective wealth by over five trillion dollars in the past three years, all thanks to Covid.
#40 – We were immediately and repeatedly told that only a vaccine could remedy the “pandemic” and get us back to normal and what is in the covid vaccines?
How in the world did people like Bill Gates, Dr. Anthony Fauci, Dr. Zeke Emanuel, and countless others know instantly that a vaccine was the only way out of the “pandemic”? I’ve explained the answer to this question in lengthy detail in my article, Beware the Vaccine Pt. 2 – The Plan to Vaccinate the Planet.
By now it should be obvious that from the outset, the entire goal of this “pandemic” has been to inoculate the entire planet with a “vaccine.” Why else would all other treatments (besides Big Pharma-backed ones like Remdesivir) be banned or vilified? Why else would there be so much pressure to roll up one’s sleeve and take the jab? Why else would there be so much propaganda regarding how “safe and effective” COVID-19 vaccines are, when there is so much evidence to the contrary?
What is in the So-called COVID-19 “Vaccines”?
Between July 2021 and August 2022, evidence of undisclosed ingredients in the COVID-19 “vaccines” was published by at least 26 researchers/research teams in 16 different countries across five continents using spectroscopic and microscopic analysis. Despite operating largely independently of one another, their findings are remarkably similar and highlight the clear and present danger that the world’s population has been lied to regarding the contents of the COVID-19 “vaccines”. This raises grave questions about the true purpose of the dangerous experimental injections that have so far been shot into 5.33 billion people (over two thirds of the human race), including children, apparently without their informed consent regarding the contents. Surprise findings include sharp-edged geometric structures, fibrous or tube-like structures, crystalline formations, “microbubbles”, and possible self-assembling nanotechnology. The blood of people who have received one or more COVID-19 “vaccines” appears, in case after case, to contain foreign bodies and to be seriously degraded, with red blood cells typically in Rouleaux formation. Taken together, these 26 studies make a powerful case for the full force of scientific investigation to be brought to bear on the COVID-19 “vaccine” contents. If the findings of these 26 studies are confirmed, then the political implications are nothing short of revolutionary: a global crime against humanity has been committed, in which every government, every regulator, every establishment media organization, and all the professions have been complicit.
Below a link which has many videos and pictures to show what is in the Covid Vaccines
https://thehardtruth.info/what-is-in-the-covid-vaccines
Scientists prove Graphene Nanobots are in the Covid Vaccines, shedding from the Vaccinated to the Unvaccinated; But there is a way to remove them

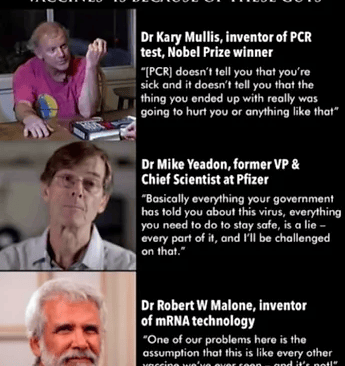
This article was originally on the websites below. But further links, pictures and videos have been added by me.
https://truthunmuted.org/40-reasons-why-a-covid-19-pandemic-never-existed-part-1/
https://www.globalresearch.ca/40-facts-you-need-to-know-the-real-story-of-covid/5813612
https://off-guardian.org/2023/03/24/40-facts-you-need-to-know-the-real-story-of-covid/
Video below: DR Mike Yeadon, a former Chief Scientific Officer with Pfizer explains in great detail why there was NO Covid-19 Pandemic